The following application is optional.
SICHC recommends filling it out, just in case you think you may be eligible.
However, if you choose to not enroll in CHAP, then proceed onto our final form —
Proof of Identity and Insurance.
About CHAP
Since 1975, Southern Indiana Community Health Care has offered financial assistance to anyone who is having difficulty paying for healthcare, and as a federally qualified community health center, we will not deny services to anyone based on their ability to pay.
SICHC’s Community Health Assistance Program (CHAP) offers a sliding fee discount for qualifying patients whose income and family size is below 200% of the federal poverty guidelines.
CHAP Benefits
- Discount for office visits at any SICHC location including a school-based health center or a school-based telehealth visit.
- Discount for lab services
- Eligible for paid transportation vouchers from Blue River Transit Services and Orange County Transit to any SICHC location
- More than Money Program – trade volunteer hours in the community for $15 toward any SICHC charges
If you have any questions, please contact Patient Accounts at (812) 723-7121.
Once this application is submitted, a representative from SICHC will contact you to help you submit additional needed forms.
Sliding Fee Discount Guidelines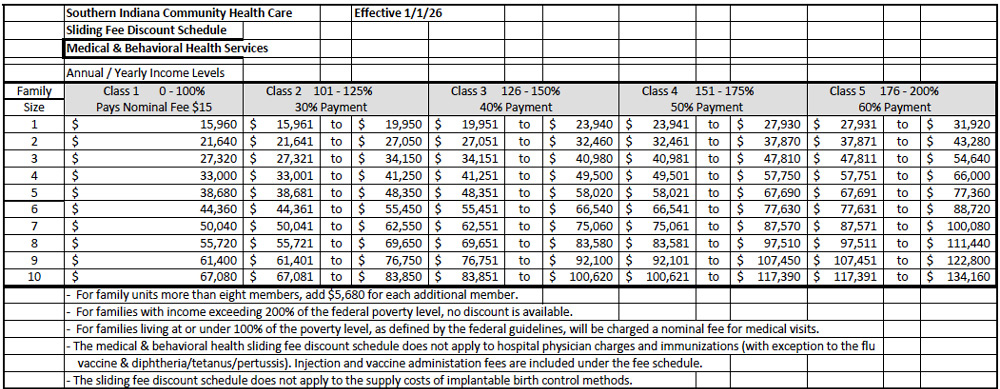
Click on the link to see additional discount guidelines for Dental and Hospital Services



